



As a sports medicine physician, I’ve seen my fair share of bad technique in the gym. Deadlifting can not only look daunting to beginners, but potentially be painful if performed incorrectly. In this post, we’ll discuss the reasons you get knee pain while deadlifting (and how to fix it).
The 8 most common reasons you get knee pain deadlifting are:
Having an excessively wide stance
Your starting position is too low
Keeping your weight too far ahead of you
Lifting the bar too fast
Locking your knees too early or excessively
Not locking your knees at the top of the deadlift
Having a rapid, uncontrolled descent
Moving your knees forward before starting to put the bar down
For each of these reasons, I’ll provide solutions so that you’re well on your way to having healthier knees when deadlifting. Let’s first discuss the anatomy of the knee and how the knee functions when deadlifting.
Need a workout program? Try Fitbod for Free.
Basic Knee Anatomy & How It Functions During Deadlifts
Let’s briefly cover the anatomy.
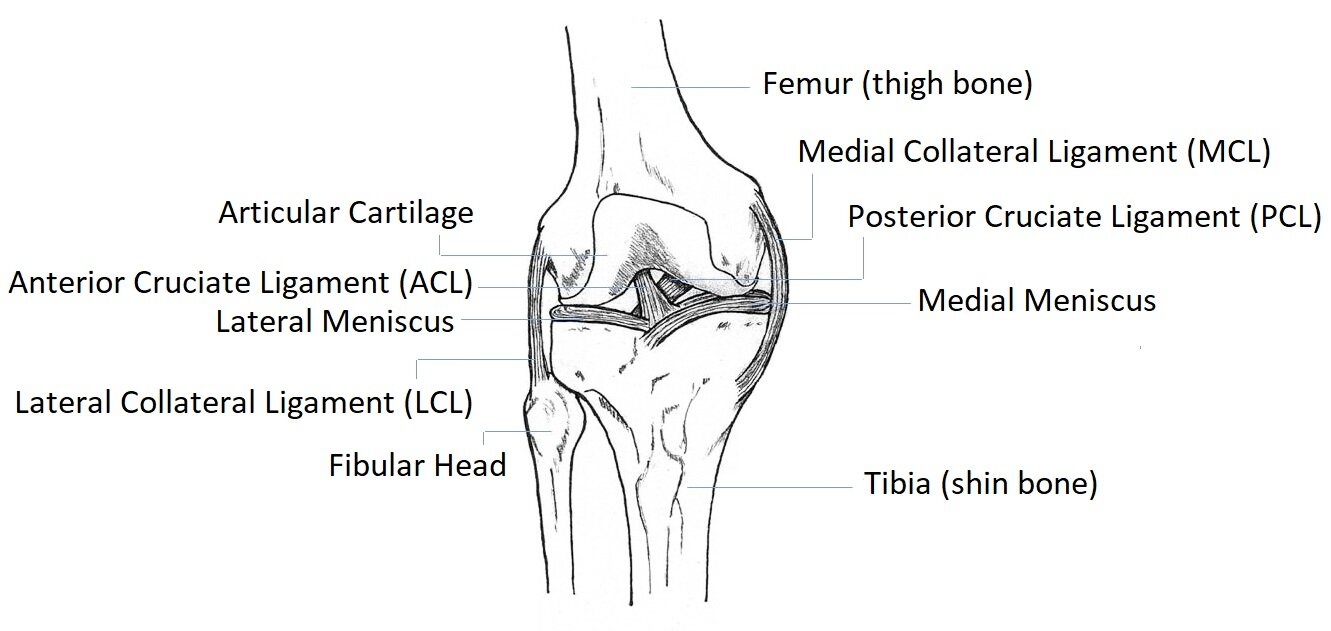
Knee anatomy
The knee joint contains four bones which are the: femur, tibia, patella, and fibula.
The thigh bone (femur) is broken up into the medial and lateral condyles, which are the edges that sit on top of the shin bone (tibia).
Both the thigh bone (femur) and shin bone (tibia) are lined with shock-absorbing cartilage which includes the lateral and medial meniscus.
The knee also has ligaments (which hold bone to bone) across both the femur (thigh bone) and tibia (shin bone) that provide stability with:
Forward (anterior) movements
Backward (posterior) movements
Outside (lateral) movements
Inside (medial) movements.
The knee cap (patella) is a bone that is a part of the quadriceps tendon that sits in a groove on top of the femur (thigh bone) and is also connected to the tibia (shin bone) through the patellar tendon.
There is a common misconception that the knee is just a hinged joint that bends (flexes) and straightens (extends). Its actual motion is much more complex due to the contours of the medial and lateral femoral condyles, which are oval-shaped and not rounded when they sit on top of the shin bone (tibia). Due to this shape, the knee joint also has a small degree of inside (medial) and outside (lateral) rotation as well.
Related Acticle: Dynamic Strength Training: 13 Exercises To Build Strength
How The Knee Functions During The Deadlift
So how does the knee functions during a deadlift?
For the sake of this article, we’ll focus on the conventional deadlift and not the sumo style deadlift. With the conventional style, there is a narrow stance with the barbell held with the hands positioned outside of the knees.

Conventional deadlifting stance
Basic Deadlifting Technique
The general technique of a deadlift starts when the bar is pulled, with straight arms, off the floor and up the legs until the knees, hips, and shoulders are locked out. With a secure grip, the knees are bent (flexed) forward with the shins just barely touching the bar.

Conventional deadlift start position
The knees are then moved out of the way (extend) slightly while keeping some contact with the shins as you begin the pull.

Keep bar over midline of foot and maintain the barbell on your shins
The bar is pulled vertically with the force of the bar being focused on the mid-foot and ending at the top at arms’ length with the chest up, hips and knee straightened (extended), the spine in a normal (neutral) position, and feet flat on the ground.

Move the knees out of the way as you drive the barbell off the floor
The knee is then locked (extended) at the top to secure the weight. The locking of the knee occurs with activation of the quadriceps (remember they’re attached to each other) which causes extension and medial rotation of the knee.

Initiate the lockout by flexing the quads and straightening the knees
When lowering the bar, the knees and hips are unlocked (flexed) in a movement opposite to that of the upward bar path. When the knee unlocks it moves into flexion and slight lateral rotation, releasing tension in the collateral ligaments to allow a smooth motion down under the influence of the hamstrings, which are a group of muscles that serve as the primary flexors of the knee.
Related Article: 7 Tips for Weight Lifting With Plantar Fasciitis
Reasons Why Your Knee Hurt While Deadlifting
IMPORTANT: We’re discussing reasons people get knee pain while deadlifting. One thing I didn’t cover was if you already have an undiagnosed knee injury you should consult a medical provider before attempting to deadlift. The last thing you’d want to do is make things worse than they are.
We briefly listed the reasons why your knee hurts while deadlifting earlier, however, let’s break it down by each phase of the deadlift
There are three phases to the deadlift: the starting phase, the pull phase, and the descent phase. By understanding each of the movements, you’ll be in a better position to spot areas of improvement to avoid knee pain.
The Starting Phase
During the starting phase, there are three things you have to avoid to help protect your knees.
Those are:
Having an excessively wide stance
Having too low of a starting position
Keeping your weight too far ahead of you
Let’s break each of these down further.
REASON #1: HAVING AN EXCESSIVELY WIDE STANCE:
An excessively wide stance can increase the compressive forces along the knee, while a stance that is too narrow can increase the forces on the knee when it locks (extends) as well. We’re trying to minimize unnecessary forces on the knee while performing the deadlift so if something as simple as making sure your starting stance is correct can prevent an injury, it’s worth doing and only takes a couple of seconds. The general rule of thumb is to stand with your feet shoulder-width apart or slightly inside shoulder width.

When your feet are too wide you may end up getting sore knees from deadlifting
REASON #2: HAVING TWO LOW OF A START POSITION
Remember this is a deadlift and not a squat. I say this because some people tend to start too low (below the hips being parallel to the ground) as their starting position. This tends to unnecessarily increase the compressive forces along the knee joint when you go into the pull phase (bring the bar up).

A hip position that is too low can cause knee pain while deadlifting
REASON #3: KEEPING YOUR WEIGHT TOO FAR AHEAD
In terms of where to keep the bar (weight), its best to have it just barely touching the shins directly over your midfoot. By keeping this position you’ll be able to direct the forces from the bar evenly over your mid-foot instead of too far ahead or behind which can add unnecessary compressive forces to the knee joint during the pull phase.

Keep the bar on you throughout the entire range of motion to reduce stress on the knee joint
2. The Pull Phase
Now that we know where things can go wrong for the knee in the start position, let’s talk about what you want to avoid in the “pull phase” in order to protect the knee.
Things you need to avoid in the “pull phase” are:
Lifting the bar too fast
Locking your knees too early or excessively
Forgetting to lock your knees at the top of the deadlift.
Let’s break each of these down further.
REASON #4: LIFTING THE BAR TOO FAST
An increased speed of movement of the bar can increase the forces on the knee joint greatly when compared to a more controlled, slower movement.

Pulling too fast off the floor can cause knee pain while deadlifting
REASON #5: LOCKING YOUR KNEES TOO EARLY
Regarding locking the knees, you want to avoid locking (extending) the knees prematurely or excessively as you can increase the forces along the patella (knee cap) or you may develop a ‘stiff-leg’ deadlift. What this will look like will locking your knees before your hips, which will cause your shoulders to be in front of the barbell when your knees begin to lock.

Locking your knees too early, where your shoulders are in front of the barbell, can cause knee pain while deadlifting
REASON #6: FORGETTING TO LOCK YOUR KNEES
At the top of the lift, you want to make sure that your knees lock. We know that the timing of the lock-out is important, i.e. not locking them too early. So what is the appropriate timing? The general rule is to lock your hips and knees at the same time. If you find that your knees are ‘soft’ and not locked, then focus on squeezing your quads, which will initiate the knee extension.

Not locking the knees in the lockout can cause knee pain while deadlifting
3. Descent Phase
Based on what you’ve read so far, these last two things to avoid will be common sense.
Avoid having:
A rapid, uncontrolled descent
Moving your knees forward before starting to put the bar down
REASON #7: AVOID A RAPID UNCONTROLLED DESCENT
Rapid and uncontrolled descent is said to produce excessive strain and force to the ligaments of the knee. This is on top of the increased compression forces that are already present in the knee when you bend (flex) the knee itself.
REASON #8: AVOID MOVING YOUR KNEES FORWARD
The reason you want to avoid moving your knees forward before starting to put the bar down is to avoid hitting your knee cap (patella). If you hit the knee cap with a loaded barbell it will cause trauma to the patella itself, which at the minimum will cause a bruise and at the maximum could lead to cartilage or bone damage.
Now that we’ve covered the specifics regarding the conventional deadlifting techniques and its relation to knee mechanics and knee pain, let’s focus on knee diagnoses and their relation to deadlifting as well.
Looking for a workout program? Try using the Fitbod App, which will design your program based on your logged training data and goals. The workouts will adapt automatically to your levels of recovery and rate of progress. With over 600 movements and exercises videos, you can be sure to perform the movements correctly for optimal results. Take the guesswork out of your workouts. Try Fitbod for free.
Tyes of Knee Pain
There are 4 types of knee pain.
1. Generalized Knee Pain:

Generalized knee pain while deadlifting
This is the type of knee pain where you can’t point to one spot on your knee that causes pain when you deadlift. The list of possibilities is endless however there are a few diagnoses that are more likely in the setting of deadlifting and those are:
Patellofemoral Syndrome: This is irritation and pain behind the kneecap (patella), specifically the cartilage, as a result of repeated bending (flexing) and straightening (extending) of the knee.
Patellar Subluxation: When there is a partial dislocation, compared to a full dislocation in a patellar dislocation, of the kneecap (patella) from its position in the groove on top of the femur (thigh bone). This can occur if you hit your kneecap with the bar.
Osteoarthritis Exacerbation: When you already have osteoarthritis present in the knee joint (bone on bone or narrowed joints) you can irritate arthritis further by adding uneven forces through the knee joint or providing too many forces.
Referred Pain: Just because you’re feeling pain in the knee, it doesn’t mean it can be from the knee directly. There are so many nerve connections in the body and a lot of them cross with each other. Sometimes when we don’t find a source of pain in the knee directly, we look for issues in the hip as well (outside the scope of this article).
2. Anterior Knee Pain

Anterior knee pain is when you get pain on the front of the knee when deadlifting
This is when asked to point to where your knee hurts when deadliting, and you point to the front of the knee. This can potentially be caused by:
Patellar Tendinopathy: It is a very generalized term for inflammation. Tendinitis is acute inflammation (seen at the level of the tissue fibers) whereas tendinosis is chronic inflammation. Tendinopathy can refer to both.
Quadriceps Tendinopathy: This is due to inflammation of the quadriceps tendon.
Hoffa’s Fat Pad Syndrome: Irritation of Hoffa’s Fat Pad which sits behind and just below your kneecap (patella), where it acts as a protective cushion, separating your kneecap (patella) from your shin (tibia) and thigh bone (femur).
Prepatellar or Infrapatellar Bursitis: Bursas are fluid-filled sacs that provide cushioning around bones, tendons, etc. People generally develop bursitis as a result of overuse or repetitive activity.
3. Medial or Lateral Knee Pain:

Medial or lateral knee pain is pain on the inside or outside of the knee
This is when asked to point to where your knee hurts when deadlifting, and you point to the inside part of my knee (closer to your inner thigh) or outer part of my knee. This can be caused by:
Acute Medial Meniscus Tear: When someone develops an acute tear of the meniscus it can be extremely painful and cause a sudden increase of pain (even if you already have baseline knee pain). These injuries are usually caused by sudden movements when the knee is under a lot of force. Deadlifting can produce a lot of forces through the knee, however, there should not be any sudden movements at the level of the knee joint itself during a conventional deadlift.
Iliotibial (IT) Band Syndrome: This is usually a cause of outside (lateral) knee pain where the IT band attaches to the shin bone (tibia).
4. Posterior Knee Pain

Posterior knee pain is pain on the back of the knee when deadlifting
This is when asked to point to where your knee hurts when deadlifting, and you point to the back of your knee. This is unlikely to be related to the knee unless there are unusually large forces. Patients commonly point to a baker’s cyst when they complain of pain in the back of the knee.
A baker’s cyst is an abnormal swelling of the bursa at the back of the knee. This can be caused by osteoarthritis, previous or current injuries, etc. You’re more likely to get pain as a result of referred pain from the hamstring or calf rather than the knee joint itself while deadlifting.
Related Article: 10 Knee Friendly Quad Exercises (Form Tips For Safe Knees)
What Should You Do When Your Knee Hurts?
There are a lot of different things you can do to help your knee when it hurts. It all depends on if the pain is acute (recent within the last 6 weeks) or chronic (generally greater than 6 weeks), but for the sake of this article we’ll cover what to do with acute knee pain, especially after deadlifting.
The first thing to do is to see if:
You’re having any loss of sensation (loss of physical feeling) in your knee or leg
Notice a markedly large decrease in your knee strength
Notice that your pain doesn’t follow the rule of twos
The Rule of Two: For the rule of twos you first rate your pain on a scale from zero to ten (zero being no pain and ten being the worst pain possible). You then note if the pain level in your knee (for example) increases by two levels (on a scale from one to ten on the pain scale) for more than two hours. If the pain increases by two levels for more than two hours, you’re doing “too” much and need to back down or be evaluated in person.
If you’re noticing any of those things then you should be seen by a medical provider as soon as possible.
Now that we know you’re not in need of immediate medical attention, let’s focus on the things we can do to when your knee hurts.
I have a few overarching principles that I like to follow in the treatment of acute joint injuries which include:
Follow PRICE
Most of you are familiar with RICE which stands for rest, ice, compress, and elevate. PRICE just adds protection to the start of the acronym. Protection can be a knee compression wrap or brace to add some support and control swelling as well.
Decrease Inflammation
One of the best non-prescription anti-inflammatories that you can use has to be ice. Generally five minutes on, and ten minutes off. If you’re looking for something more than ice, your medical provider can help you decrease inflammation through medication by mouth or even a steroid injection into the knee joint.
Decrease activity and use training modifications (includes assessing technical issues)
While the inflammation in the knee is being controlled, it’s also a good idea to avoid activities that could flare it up again or make it worse. This is done by avoiding activities that reproduce the pain which is easy and goes back to the old saying “if it hurts to do that, don’t do it.”
Over time, increasing range of motion (ROM) and strength back to baseline and beyond
The final step after controlling the inflammation is bringing your knee ROM and strength back to where it was prior to the injury and start strengthening it beyond that level. This can be performed by first checking ROM while on a stationary bike, then progress with walking, jogging, and running (with varying intensities). Once ROM and strength have been established to be back at baseline AND there is very little to NO pain (as minimal as possible), it’s a good time to start increasing your strength beyond this level, and of course, continue to deadlift.
Final Thoughts
The deadlift is an excellent strengthening exercise that can not only look daunting to beginners but potentially be painful if performed incorrectly. You can avoid or limit the reasons you get knee pain while deadlifting by making small adjustments to your technique and ensuring that you treat acute knee pain appropriately before getting back in the gym.
About The Author

Dr. Niraj Patel is a physician and assistant professor of family medicine and sports medicine at the University of North Texas Health Science Center. He completed his family medicine residency training through Cleveland Clinic Akron General where he served as the Chief Resident and House Staff President. He completed his sports medicine fellowship through Ohio Health Riverside Methodist Hospital; team physicians of the Columbus Blue Jackets (NHL) and the Columbus Crew (MLS). In addition, he has completed a Certificate in The Principles of Aviation & Space Medicine through NASA / The University of Texas Medical Branch where his final project was on the topic of “Muscle Loss in Spaceflight.” Niraj has been published in the Clinical Journal of Sports Medicine as well as Current Sports Medicine Reports, the official review journal of the American College of Sports Medicine. In his spare time, Niraj enjoys reading, working out, watching sports (especially hockey), and spending time with his family.
References
Bengtsson, B., Berglund, L., Aasa, U. 2018. Narrative review of injuries in powerlifting with special reference to their association to the squat, bench press, and deadlift. BMJ Open Sports Exercise Medicine.
Escamilla, R. 2001. Knee biomecchanics of the dynamic squat exercise. Medicine Science Sports Exercise, 33(1): 127-141.
Escamilla, R., Francisco, A., Fleisig, G., Barrentine, S., Welch, C., Kayes, A., Speer, K., Andrews, J. 2000. A three-dimentional biomechanical analysis of sumo and conventional style deadlifts. Medicine Science Sports Exericse, (7): 1265-1275.
Hattin, H., Pierrynowski, M., Ball, K. 1989. Effect of load, cadence, and fatigue on tibio-femoral joint force during a half squat. Medicine Science Sports Exercise, 21(5): 613-618.
Schoenfeld, B. 2010. Squatting kinematics and kinetics and their application to exercise performance. Journal of Strength and Conditioning Research (12): 3497-3506.
Shankman, G. 1984. Training related injuries in progressive resistive exercise programs. National Strength and Conditioning Association Journal, 6(4): 36-37.




